
Where I started: open hernia repair
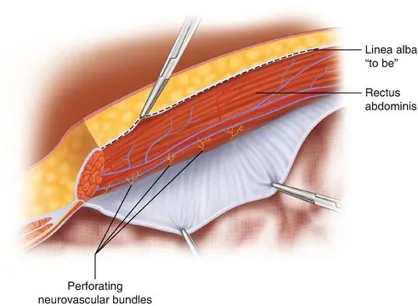
I feel the best place to put mesh is either underneath the rectus muscle or between the rectus fascia and the peritoneum. When I first started performing hernia repair, it was 2008, and I performed most of my cases in an open fashion, which let me get good mesh placement in that space between the rectus muscle and the fascia above it. Results were good.

As time went on, I started seeing more hernias like the one above — not always huge, but ones that definitely needed repair. At the time, open surgery was the best tool I had for this type of hernia.
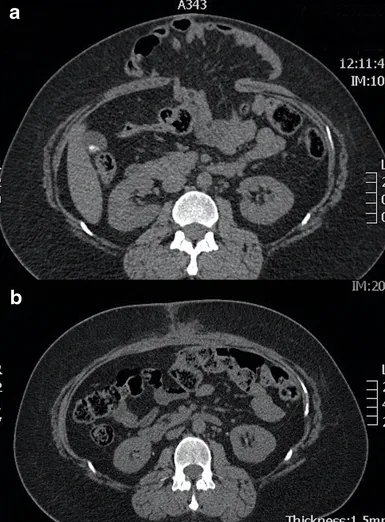
The CT scans above show two images. The top shows a fairly large hernia containing intestine. The bottom shows a strong repair, where the rectus muscles have been brought back together in the midline. I still feel this is the best kind of repair to offer patients — it doesn't just get rid of the hernia, it restores normal core function, which can lead to better posture and balance.
Minimally invasive (MIS) robotic-assisted abdominal wall hernia repair techniques started being discussed in the mid-2010s. Knowing the benefits of MIS surgery, I became intrigued. I felt it would be great to be able to restore my patients' core through an MIS approach.
Teaching while the field changed

Like today, much of my practice back then involved teaching residents. I was performing MIS surgery, but it was mostly limited to gallbladder disease and inguinal hernias. The photo above is from that era — the surgeon on the left is pointing to the monitor, demonstrating surgical anatomy and technique. It could get a bit tedious having to keep reaching back to point during an operation.
Adopting robotic surgery

As general surgeons began adopting robotic-assisted surgery, as new hernia repair techniques were refined to allow mesh placement directly into the abdominal wall, and as my desire grew to bring the benefits of MIS surgery to my patients and modern surgical education to residents, I began incorporating robotic-assisted surgery into my practice.
My initial training was in January 2020, and my first three cases — one cholecystectomy and two inguinal hernias — happened within a single week. For me, adopting robotic surgery wasn't about learning how to operate. It was about bringing new technology into the operating room to perform cases I already knew how to do.
Where I am today

Not every case is right for a robotic approach. I treat each patient as an individual and tailor my operative approach to their specific circumstances. But today, I perform robotic-assisted MIS cases as often as I safely can.
With robotic surgery, the benefits to patients are noticeable: earlier discharge home, less post-operative pain, less wound care, and a faster return to work.
Robotic approaches benefit your surgeon, too. A few examples: the cameras provide 3D, high-definition images that let us see down to the capillary level in some cases; wristed instruments inside the abdomen allow precise surgical movement that mimics the human hand; and on-screen pointers let me demonstrate technique to residents without reaching back across the room.
As of May 2026
I've performed over 1,200 robotic cases, including more than 200 in each of the last three years: