
The short version
- Classic gallbladder pain hits after fatty meals — upper right abdomen, sometimes spreading to the back or right shoulder blade.
- Painful stones, inflammation, or a gallbladder that empties poorly (confirmed by HIDA scan) are the usual reasons to remove it.
- Removal is typically same-day ; most people return to work in 1–2 weeks.
- There is no permanent diet afterward — most people eat normally within a few weeks.
A quick summary — the full details are below, and none of it replaces an exam.
What does the gallbladder do?
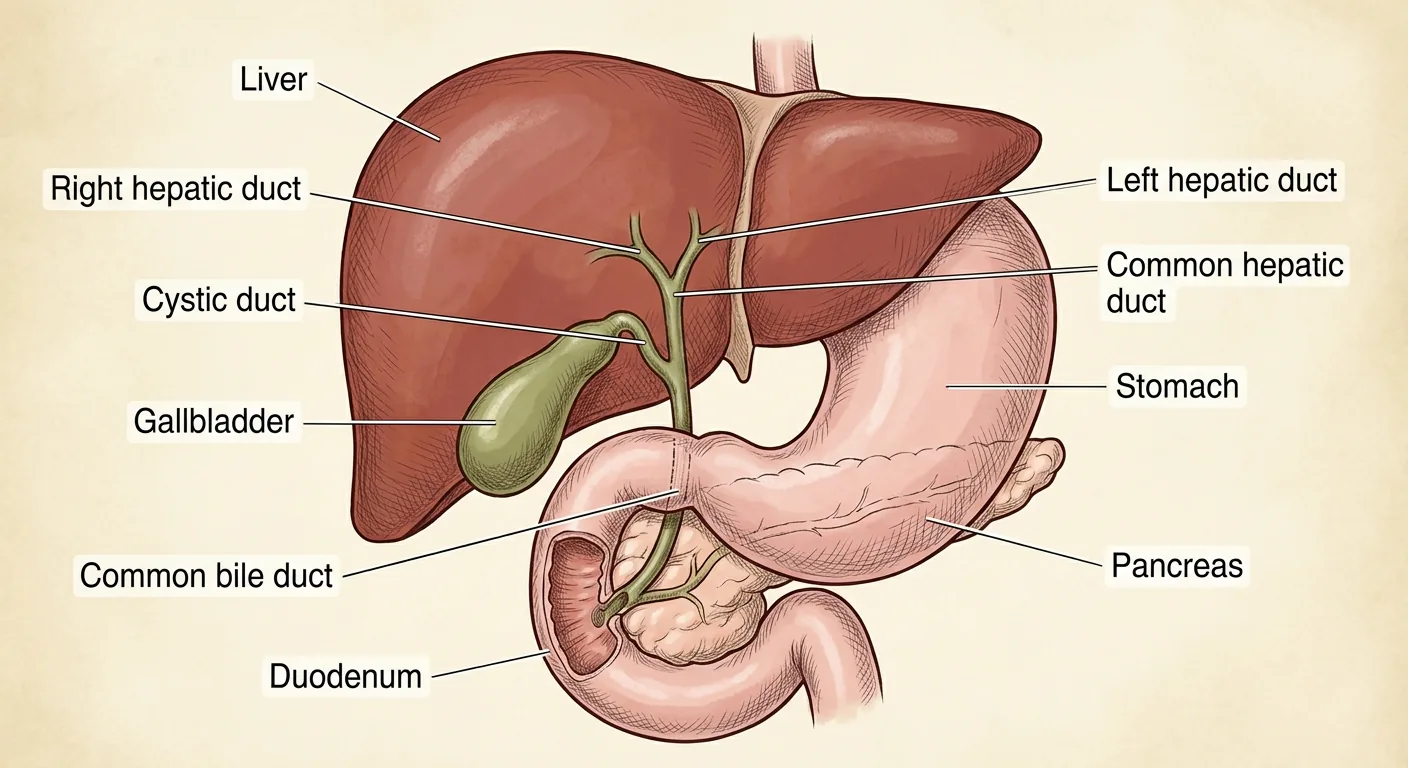
Your liver makes a fluid called , which helps your body break down fat from food. Your gallbladder is a small sac that stores and concentrates that bile. After you eat, especially something fatty, your gallbladder squeezes and sends bile down a tube (the ) into your small intestine, where it mixes with food and helps digestion.
If a stone blocks that tube, bile can't get out. The pressure builds up inside the gallbladder, and that's what causes pain.
How do gallstones form?
are hard little particles that form inside the gallbladder when the bile is out of balance. There are three kinds:
- Cholesterol stones: the most common type. There's too much cholesterol in the bile, and not enough of the substances that keep it dissolved, so it crystallizes into a stone.
- Pigment stones: made from bilirubin, a substance left over when red blood cells break down. Certain blood disorders or liver problems raise the risk.
- Mixed stones: a combination of both.
What about GLP-1 medications like Ozempic or Wegovy?
GLP-1 medications, used for diabetes and weight loss, can slow down how well your gallbladder empties. Combined with rapid weight loss, this raises your risk of forming gallstones. If you're on one of these medications and develop upper-abdomen pain after meals, it's worth getting checked.
What does gallbladder pain feel like?
Classic gallbladder pain (called ) shows up after a fatty meal. It's usually felt in the upper right part of your abdomen, and it can spread to your back or right shoulder blade. If a stone stays stuck, the gallbladder can become inflamed or infected (a condition called cholecystitis), or a stone can travel further and cause , a bile duct infection, or . Any of these need prompt medical attention.
What if my scans don't show stones, but I still have the pain?
Some people have all the same symptoms without any visible stones. This is called biliary dyskinesia: the gallbladder isn't squeezing or emptying properly. We diagnose this with a HIDA scan, a test that measures how well your gallbladder empties. If emptying is poor and your symptoms match, removing the gallbladder is often still the right answer.
When is gallbladder removal recommended?
- Painful gallstones (symptomatic cholelithiasis)
- Gallbladder inflammation (cholecystitis)
- Gallbladder polyps larger than 1 cm, or growing on repeat ultrasounds
- Biliary dyskinesia (poor emptying, confirmed by HIDA scan)
- Biliary hyperkinesia (excessive emptying, confirmed by HIDA scan)
- Gallbladder infection
- Stones that have moved into the main bile duct (choledocholithiasis)
- Gallstone pancreatitis
How robotic-assisted repair works
During robotic surgery, Dr. Rodriguez sits at a console near the operating table and controls every robotic instrument directly, while the surgical team stays at your side throughout. The robotic system provides a high-definition, 3D view inside your abdomen, allowing precise movement through just a few small incisions.
- Anesthesia: you're fully asleep for the entire procedure.
- Getting in: usually four small incisions are made. Entry into the abdomen is done with a see-through device, so each layer of the abdominal wall is identified as it's entered. Once inside, the abdomen is gently filled with air, and the area right below the entry point is checked to confirm the colon, small intestine, and stomach weren't injured.
- Robotic setup: robotic arms are connected to the instruments placed through those incisions.
- Removal: the gallbladder is carefully freed and removed.
- Closure: incisions are closed with stitches and surgical glue.
How does Dr. Rodriguez reduce risk during surgery?
Every operation has some risk. Here's specifically what's done to lower it:
- Critical View of Safety: the key structures (cystic duct and cystic artery) are clearly identified and freed of surrounding tissue before anything is cut, which is the single biggest safeguard against bile duct injury.
- Fluorescent cholangiography: a green dye, given through an IV before surgery, glows under special light so the bile duct anatomy is visible in real time.
- Intraoperative cholangiogram: an X-ray dye study, used selectively, to confirm anatomy and rule out retained stones.
- High-definition 3D visualization from the robotic system itself.
- Continuous monitoring of your vital signs throughout the case.
Risks to know about
- Bleeding or infection
- Injury to nearby organs (liver, intestines, blood vessels)
- Injury to intestines, blood vessels, or nerves during initial entry and during the dissection process. This risk is small, but does vary based on anatomy and scar tissue
- Injury to the bile duct system, or a bile leak
- Blood clots
- Reaction to anesthesia
- Need to convert to an open operation
- Pain at the incision used to remove the gallbladder (usually just left of the navel)
- Loose stools after surgery
Why does diarrhea happen after gallbladder removal?
Once the gallbladder is gone, there's no longer a storage tank for bile. Instead, it trickles continuously from the liver into your intestine. That steady trickle can act like a mild laxative for some people. It's usually mild and improves with time; diet changes or medication can help if it doesn't.
Recovery: what to expect
- Hospital stay: most patients go home the same day.
- Pain control: a mix of Tylenol (acetaminophen), Celebrex (celecoxib), Robaxin (methocarbamol), and an opioid like Ultram (tramadol) or Roxicodone (oxycodone) if needed, for about 3 days.
- Diet: start with clear liquids, then return to your normal diet. Add fatty foods back gradually, since you no longer have a bile reservoir.
- Activity: light activity right away; avoid heavy lifting for a few weeks.
- Wound care: you can shower the day of surgery. Incisions are closed with surgical glue, so keep them dry and pat (don't rub) after showering. Do not submerge incisions in a pool, tub, or other body of water for at least 4 weeks, and keep them out of direct sun for 6 months to avoid discoloration.
- Back to normal life: most people return to work within 1–2 weeks.
- Fever over 101°F, or chills
- Redness, swelling, or drainage from an incision
- Severe abdominal pain
- Persistent nausea or vomiting
- Yellowing of your skin or eyes
If it's after hours, your call will be routed to our answering service. The on-call surgeon or PA will receive your message and contact you.
For uncontrolled pain, shortness of breath, chest pain, or inability to keep fluids down, seek urgent medical attention right away rather than waiting for office hours.
Want to see it in action?
This video shows footage from an actual surgery. Viewer discretion is advised.